Parkinson’s Disease Psychosis (PDP): An Important Nonmotor Manifestation of Parkinson’s Disease
Burden and Clinical Manifestations
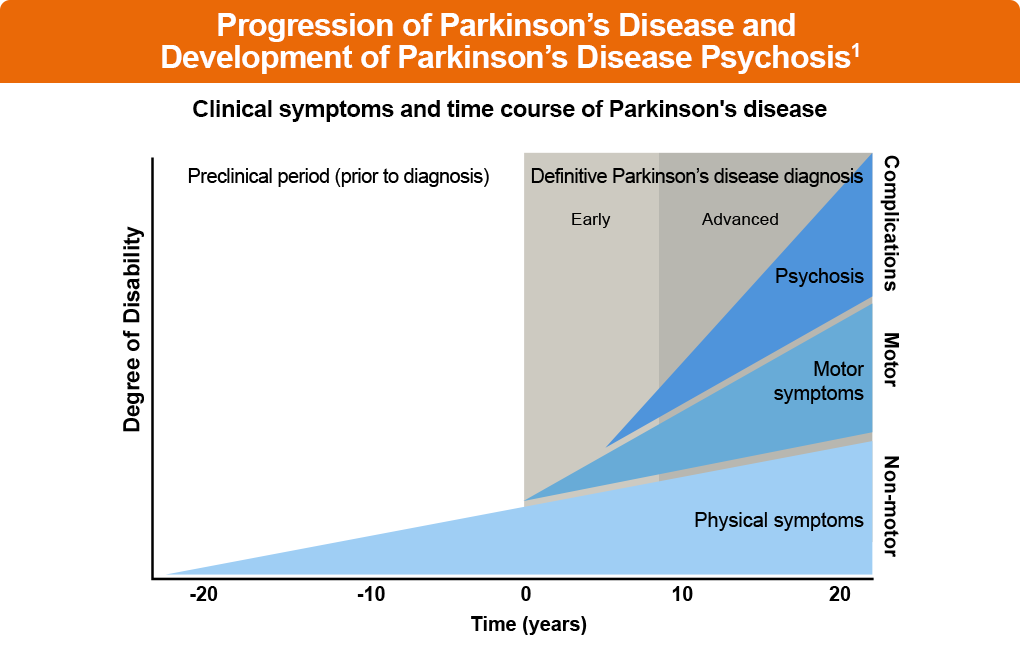
PDP is an important complication of Parkinson’s disease that accompanies progressive motor and nonmotor symptoms (Figure 1)1
This nonmotor complication of Parkinson’s disease affects an estimated 30% to 60% of the roughly 1 million patients in the United States with Parkinson’s disease1-3
Manifestations of PDP may include hallucinations, including those of a nonvisual character that may be auditory, tactile, gustatory, or visceral in nature3-5
PDP is also characterized by delusions, which are a form of disordered thinking that involves firmly held beliefs not based in reality3-5
The features of PDP are based in the neurochemistry of Parkinson’s disease6
Figure 1: Progression of Parkinson’s Disease and the Development of Parkinson’s Disease Psychosis1
Pathophysiology of PDP
Multiple neurotransmitters are involved in the pathophysiology of PDP, including dopamine, acetylcholine, norepinephrine, and serotonin, as well as the imbalanced expression of these neurotransmitters in specific areas of the brain6-10
PDP may also relate to the accumulation of misfolded proteins in certain brain regions, such as the hippocampal, frontal, and parietal regions7
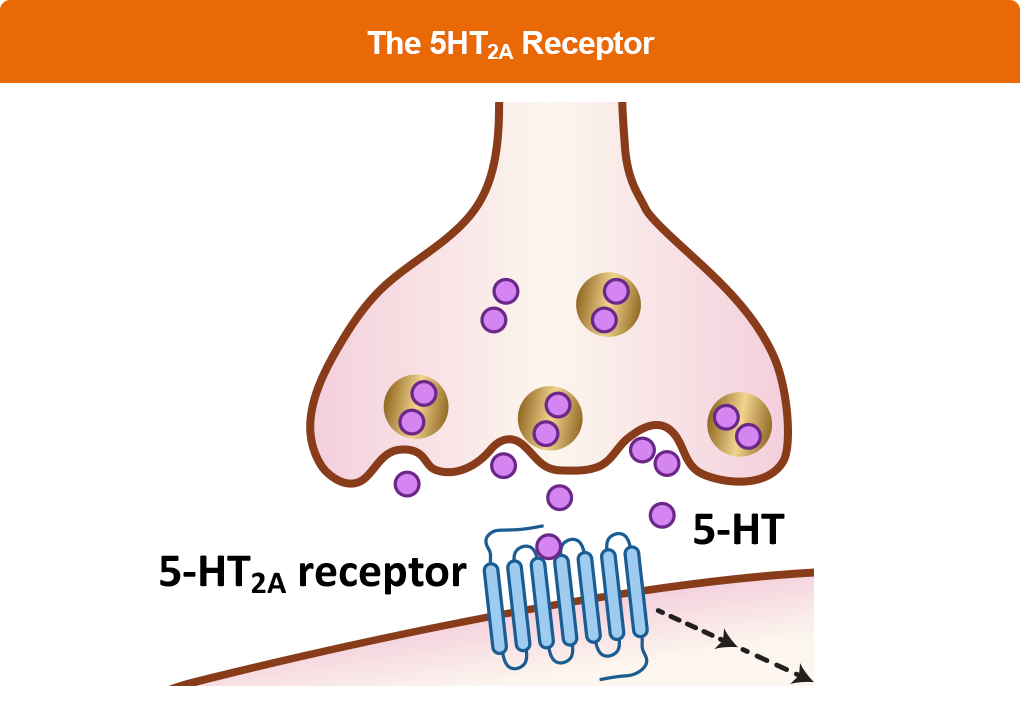
The role of serotonin 2A receptors (5HT2A) in the brain is a crucial element of the pathophysiology of PDP, and is thought to have an important role in induction of hallucinations in patients with PDP5, 11
In support of this hypothesis, an autoradiographic binding study found that 5HT2A receptors were upregulated by 46% in visual processing regions of the brain in patients with PD who had experienced visual hallucinations12
Figure 2: The 5HT2A Receptor
Treatment of PDP
The use of second generation antipsychotics for PDP could worsen their symptoms of Parkinsonism because of its ability to block multiple receptors such as the dopamine 2 receptor11,13-15
Other off-target effects of antipsychotics such as blockade of the histamine 1 receptor, alpha receptors, or muscarinic receptors may lead to off-target effects, which may increase the potential for adverse events and side effects11,13,14
In the development of pimavanserin, scientists addressed the off-target effects of previous antipsychotic medications and developed a unique medication that was specifically targeted at the 5HT2A receptor and eliminated off-target effects of the dopamine 2 receptor, histamine 1 receptor, alpha receptors, and muscarinic receptors11,13,14
In addition, scientists designed pimavanserin with a unique pharmacologic action of inverse agonist activity at the 5HT2A. Inverse agonist activity goes beyond the effect of a normal antagonist; it blocks agonists and also reduces the baseline ordinary signaling that occurs in the absence of an agonist13
Finally, unlike antipsychotic medications that were previously used off-label for PDP, such as clozapine or quetiapine, pimavanserin is specifically approved by the US Food and Drug Administration for PDP management
D2 = dopamine type 2; H1 = histamine 1 receptor; Alpha = adrenergic-alpha receptor; M = muscarinic receptor.
Fénelon G, Soulas T, Zenasni F, Cleret de Langavant L. The changing face of Parkinson’s disease-associated psychosis: A cross-sectional study based on the new NINDS-NIMH criteria. Mov Disord. 2010;25:763-766. doi:10.1002/mds.22839
Ravina B, Marder K, Fernandez HH, et al. Diagnostic criteria for psychosis in Parkinson’s disease: Report of an NINDS, NIMH work group. Mov Disord. 2007;22:1061-1068. doi:10.1002/mds.21382
Thanvi BR, Lo TC, Harsh DP. Psychosis in Parkinson’s disease. Postgrad Med J. 2005;81:644-646. doi:10.1136/pgmj.2004.032029
Klein JC, Eggers C, Kalbe E, et al. Neurotransmitter changes in dementia with Lewy bodies and Parkinson disease dementia in vivo. Neurology. 2010;74:885-892. doi:10.1212/WNL.0b013e3181d55f61
Holmqvist S, Chutna O, Bousset L, et al. Direct evidence of Parkinson pathology spread from the gastrointestinal tract to the brain in rats. Acta Neuropathol. 2014;128:805-820. doi:10.1007/s00401-014-1343-6
Lenka A, Hegde S, Jhunjhunwala KR, Pal PK. Interactions of visual hallucinations, rapid eye movement sleep behavior disorder and cognitive impairment in Parkinson’s disease: A review. Parkinsonism Relat Disord. 2016;22:1-8. doi:10.1016/j.parkreldis.2015.11.018
Combs BL, Cox AG. Update on the treatment of Parkinson’s disease psychosis: Role of pimavanserin. Neuropsychiatr Dis Treat. 2017;13:737-744. doi:10.2147/NDT.S108948
Huot P, Johnston TH, Darr T, et al. Increased 5-HT2A receptors in the temporal cortex of parkinsonian patients with visual hallucinations. Mov Disord. 2010;25:1399-1408. doi:10.1002/mds.23083
Hacksell U, Burstein ES, McFarland K, Mills RG, Williams H. On the discovery and development of pimavanserin: A novel drug candidate for Parkinson’s psychosis. Neurochem Res. 2014;39:2008-2017. doi:10.1007/s11064-014-1293-3
The THRIVE Patient Toolkit is a resource center for patients who received diagnosis of or who are interested in learning about Parkinson’s disease. Choose from the options below to learn more.
The THRIVE Clinical Toolkit is an online tool that aims to provide clinicians up-to-date information on the presentation, prognosis, pathophysiology, and treatment strategies for Parkinson’s disease. Click on one of the options below to learn more about PD.
The THRIVE Patient Toolkit is a resource center for patients who received diagnosis of or who are interested in learning about Parkinson’s disease. Choose from the options below to learn more.
The THRIVE Clinical Toolkit is an online tool that aims to provide clinicians up-to-date information on the presentation, prognosis, pathophysiology, and treatment strategies for Parkinson’s disease. Click on one of the options below to learn more about PD.