At present, there is no effective diagnostic test for Parkinson’s disease (PD), and diagnosis is based primarily on medical history and neurological exam. PD is often a diagnosis of exclusion; clinicians sometimes request brain scans or laboratory tests to rule out other diseases.1
Unfortunately, current diagnostic modalities in PD are limited by the fact that they identify PD by the presence of motor symptoms. The problem is, by the time of diagnosis, more than 60% of all dopaminergic neurons within specific regions of the basal ganglia may have been lost.2 One study suggests that an approximate loss of half of the dopamine neurons in the posterior putamen was required for symptoms to begin to manifest, based on PET scans in patients with “early” PD.3 Other studies suggest that there is a reduction in neurons of 66%,4 and near complete neuronal depletion in the putamen.4 The widely held assumption is a dopamine neuronal loss of 60% to 80%, at which symptomatic disease occurs.5
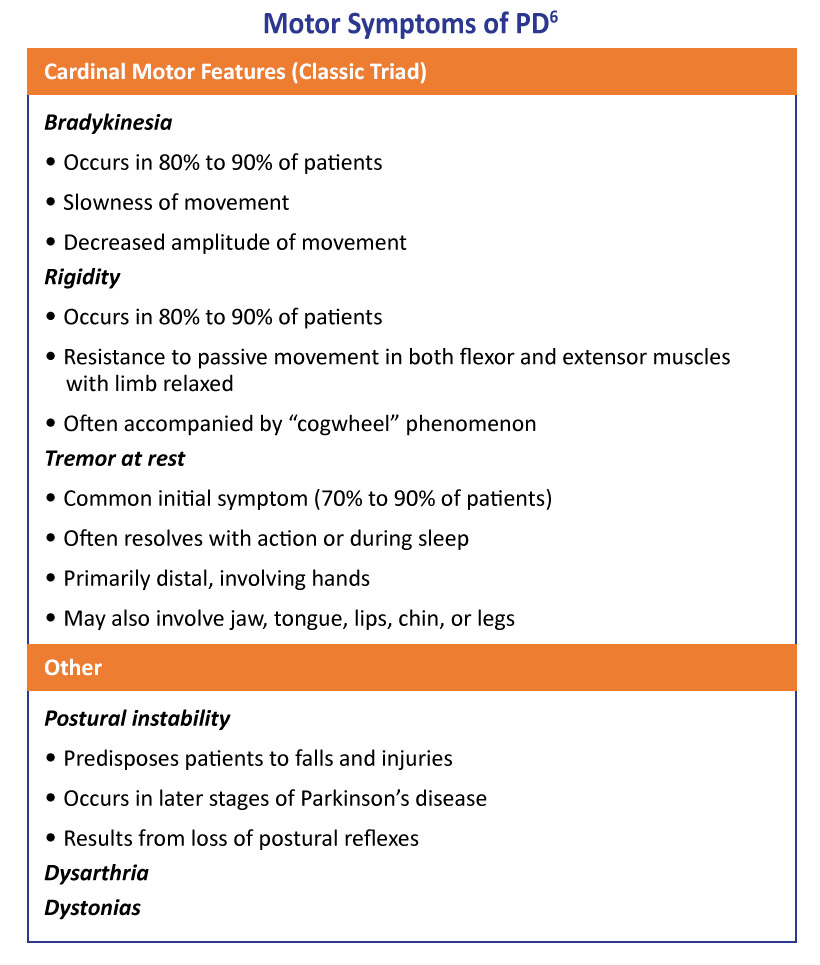
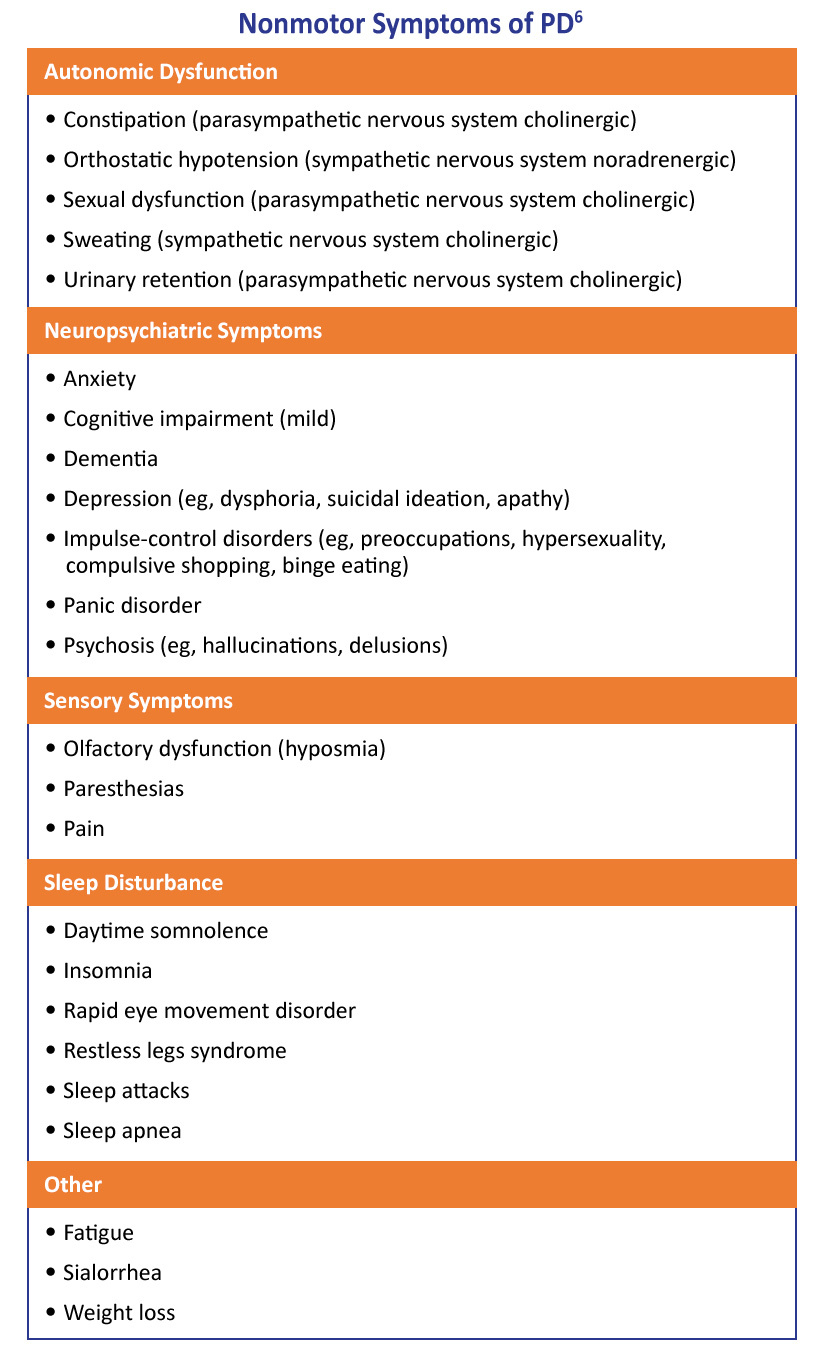
While the differential diagnosis of PD should include a comprehensive history and physical examination, difficult or questionable cases should be promptly referred to a movement-disorder specialist for further evaluation.6 A list of the most common motor and nonmotor symptoms are depicted in Tables 1 and 2 below.
Diseases/Conditions That Can Mimic Parkinson’s Disease6
Pagan FL. Improving outcomes through early diagnosis of Parkinson’s disease. Am J Manag Care. 2012;18(7 suppl):S176-S182.
Guttman M, Burkholder J, Kish SJ, et al. [11C]RTI-32 PET studies of the dopamine transporter in early dopa-naïve Parkinson’s disease: Implications for the symptomatic threshold. Neurology. 1997;48:1578-1583.
Kish SJ, Shannak K, Hornykiewicz O. Uneven pattern of dopamine loss in the striatum of patients with idiopathic Parkinson’s disease. Pathophysiologic and clinical implications. N Engl J Med. 1988;318:876-880.
Dauer W, Przedborski S. Parkinson’s disease: Mechanisms and models. Neuron. 2003;39:889-909.
DeMaagd G, Philip A. Parkinson’s disease and its management: Part 1: Disease entity, risk factors, pathophysiology, clinical presentation, and diagnosis. P T. 2015;40:504-510.
The THRIVE Patient Toolkit is a resource center for patients who received diagnosis of or who are interested in learning about Parkinson’s disease. Choose from the options below to learn more.
The THRIVE Clinical Toolkit is an online tool that aims to provide clinicians up-to-date information on the presentation, prognosis, pathophysiology, and treatment strategies for Parkinson’s disease. Click on one of the options below to learn more about PD.
The THRIVE Patient Toolkit is a resource center for patients who received diagnosis of or who are interested in learning about Parkinson’s disease. Choose from the options below to learn more.
The THRIVE Clinical Toolkit is an online tool that aims to provide clinicians up-to-date information on the presentation, prognosis, pathophysiology, and treatment strategies for Parkinson’s disease. Click on one of the options below to learn more about PD.