Levodopa and Carbidopa
Levodopa (L-dopa) is commonly given to regulate dopamine levels in patients with PD. Since its introduction in 1967, L-dopa has persisted as the gold standard for PD treatment and is an important element of combination therapies. Unfortunately, L-dopa tends to lose efficacy over time, with greater than 80% of patients on therapy for longer than 10 years experiencing symptoms.1,2 Carbidopa is often given in combination to increase dopamine exposure, allowing lower doses of L-dopa to maintain efficacy while reducing side effects such as nausea.2
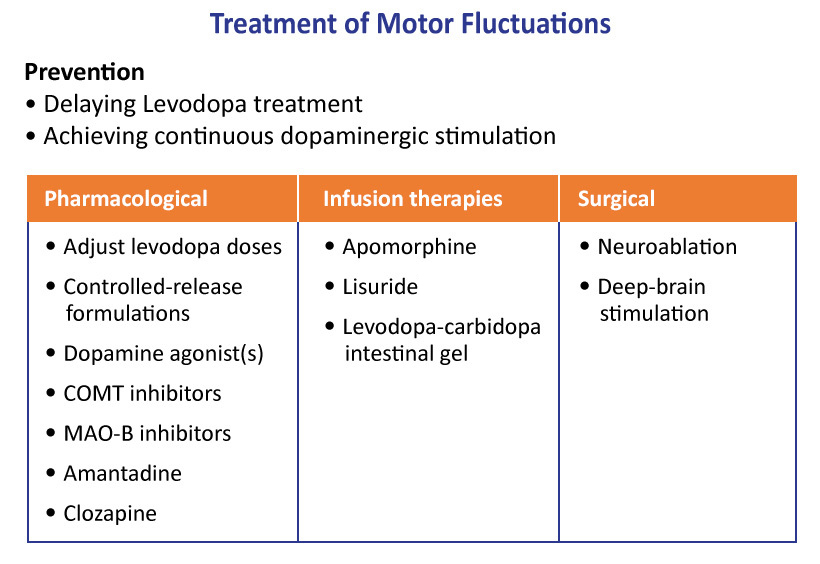
Continuous dopaminergic stimulation is a new strategy aimed at decreasing motor fluctuations in advancing PD. Three device-aided treatments are currently available to provide different kinds of continuous stimulation: levodopa/carbidopa intestinal gel infusion, deep brain stimulation (DBS), and subcutaneous apomorphine pump infusion (not approved in US).
Dopamine Agonists
Dopamine agonists act on dopamine receptors to increase the effects of dopamine. These medications include apomorphine, bromocriptine, ropinirole, pramipexole, and rotigotine.3
MAO-B Inhibitors
Monoamine oxidase B (MAO-B) is an enzyme involved in breaking down dopamine.4 MAO-B inhibitors help stop this process to increase dopamine levels. MAO-B inhibitors include selegiline, rasagiline, and safinamide.
COMT Inhibitors
COMT (catechol-O-methyltransferase) is another enzyme involved with decreasing dopamine levels. Similar to MAO-B, inhibition of COMT leads to an increase of brain dopamine levels and reduction of motor symptoms.2 Entacapone and tolcapone are COMT inhibitors now used as components of PD care.
Other Agents/Targets
Anticholinergics do not act directly on the dopaminergic system, but instead regulate acetylcholine, which is involved in regulating movement. They can have beneficial impacts on tremor and dystonia (involuntary muscle contractions) in people with PD.2 Benzatropine and trihexyphenidyl are two approved antiparkinson therapies that decrease the activity of acetylcholine. Other agents used to treat various symptoms of PD include amantadine, droxidopa, pimavanserin, and rivastigmine.